

)
)
)
)
Business Philosophy12 Aug 2025
Maziar Mike Doustdar: Novo Nordisk's New CEO
A portrait of the pharmaceutical giant's new CEO, who assumes the position at a critical time for the company in its competition with Eli Lilly.
When Danes talk about their country, they often do so by referring to Denmark as “et lille land”, translated to “a small country” in English. This can be used to explain why they might have limited leverage in some geopolitical questions, while other times it's used beaming with pride after a national athletic achievement against all odds. While Denmark may be small, its impact on the global business stage is massive compared to its size, and in the modern era, no company better exemplifies this than Novo Nordisk. From groundbreaking work with insulin to leading the charge in fighting obesity, this is the story of how tiny Denmark created one of the world's largest pharmaceutical companies.
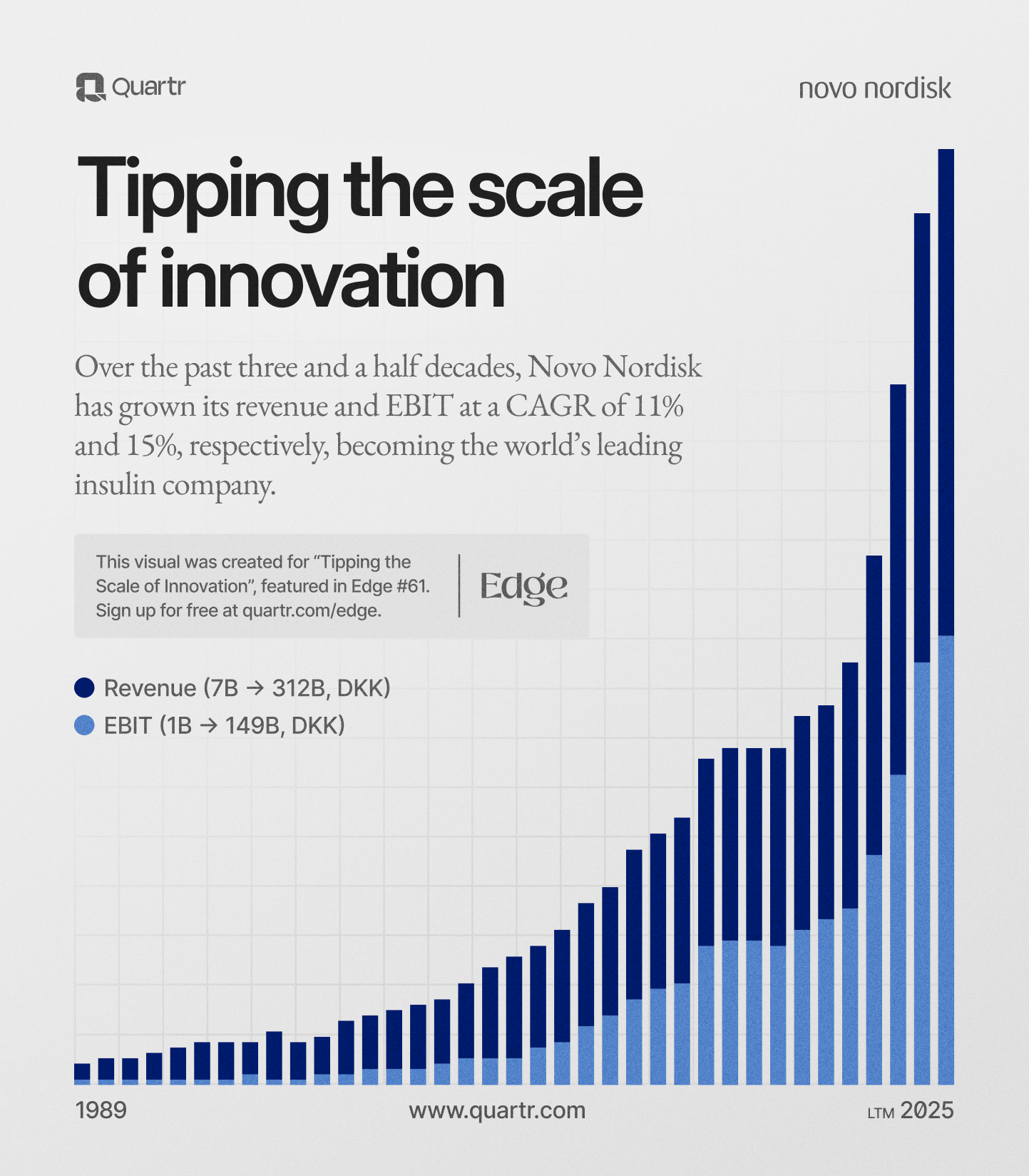
Before we begin our telling of Novo Nordisk's history, we want to take a moment to showcase just how impressive the company's growth has been since the two companies merged in 1989:
The story begins in 1922 on a ship sailing across the Atlantic Ocean bound for the U.S. Traveling onboard is one of this story's protagonists: the Danish physiologist August Krogh, accompanied by his wife Marie. Krogh had won the Nobel Prize for medicine in 1920 for his work on methods for accurately measuring blood oxygen levels, and was about to go on a lecture tour to the most prestigious universities in North America.
At first glance, everything seems to be perfect for the couple. A Nobel Prize (and the prize money) in hand, happily married, and about to go on what we assume was to be a well-paid lecture tour. But in reality, Marie was a woman living on borrowed time. She was living with a condition then referred to in Denmark as sugar disease, but which we today know as diabetes. Marie had been diagnosed in late 1921, during a time when life expectancy in years following diagnosis was one to three years.

But luckily for her, and for everyone else across the world living with diabetes, two researchers in Canada had just made a discovery that would save countless lives. On Marie's initiative, the Kroghs made a detour to Toronto to meet with Frederick Banting and Charles Best, who had just discovered how to extract and manufacture insulin. Banting's team granted Krogh permission to manufacture insulin in Scandinavia, and upon returning back home to Denmark, he joined forces with Christian Hagedorn, a diabetes specialist, and pharmacist August Kongsted.
In 1923, they founded the Nordisk Insulinlaboratorium in Copenhagen and started treating the first patients in Denmark. The business was established within a foundation structure, in line with the agreement with the researchers in Canada. The belief, both in Toronto and in Copenhagen, was that part of the profits from medicine should fund scientific and humanitarian efforts. This culture of “profit with purpose” has been a core part of Novo Nordisk's identity ever since.
As Nordisk was rapidly ramping up production, internal tensions were about to boil over. In 1924, a disagreement led Christian Hagedorn to dismiss Thorvald Pedersen, a talented chemist working in his lab. Thorvald's brother Harald, who also worked at Nordisk but on Krogh's team, handed in his resignation in solidarity. According to the people involved in what we can only assume was a somewhat tense exit interview, this is what was said:
August Krogh: “What are you going to do?”
Harald Pedersen: “We want to make insulin.”
August Krogh: “Well, you'll never manage that.”
Harald Pedersen: “We will show you!”
We don't have any more records about what happened following this exchange and whether or not hands were shaken, but the Pedersen brothers were determined to keep their promise. In 1925, they would go on to set up the Novo Terapeutisk Laboratorium (Novo is latin for “new”).
By the mid-1920s, the small country of Denmark had two fledgling insulin producers competing against each other, and a fierce yet incredibly fruitful rivalry was initiated. Both companies were driven by the same purpose and selling the same product, yet two distinct internal cultures and approaches were developed. Nordisk had academic weight and clinical focus, while Novo was fueled by entrepreneurial spirit. But the companies had two things in common: they aimed to improve insulin and save lives, and they wanted to outdo the other.
The competition (and the fact that there was now a life-saving drug available on the market) helped spur remarkable early growth. By 1931, Novo had moved out of a basement lab into a large facility in a converted dairy plant, and was, just six years after its founding, selling insulin in 40 countries. Pancreatic glands (used in the manufacturing of insulin) were being sourced from all over Europe, and both Novo and Nordisk were shipping out insulin as fast as humanly possible.
But neither of the two companies was happy with just supplying insulin to patients in need; they also wanted to understand the disease their drugs were treating. In 1932, Nordisk established the Steno Memorial Hospital for diabetes care, while Novo opened the Hvidøre Diabetes Sanatorium in 1938 to treat patients and conduct clinical research. Where one went, the other followed.
In the early morning of April 9th, 1940, German troops breached Denmark's southern border, paratroopers captured infrastructure, and the Kriegsmarine sailed into Copenhagen with battle flags flying. While the Danes put up fierce resistance, there was very little they could do to ward off the Nazi war machine. Just hours after the first shots had been fired, and following ferocious fighting in the streets of Copenhagen, Denmark surrendered.
When the workers at Novo and Nordisk went to work the next morning, they did so in an occupied city, and their employers had to adapt. Even if Europe was engulfed in war, people still needed insulin. Animal pancreases were in short supply, and Novo sought solutions that could utilize every part of the glands.
The company began extracting a digestive enzyme called trypsin after insulin was removed, which would then be used in various industrial settings. It was Novo's first step into the enzyme industry, and proved so successful that the company would eventually become a world-leading enzyme producer. The company also experimented with producing penicillin during the war, but it was not until later (after a visit to the U.S.), that Novo began producing penicillin at a large scale.
Denmark was eventually liberated, and both Novo and Nordisk could shift away from survival mode back into full focus on researching and growing. One year after the war ended, Nordisk's Christian Hagedorn made a major breakthrough. He discovered that adding a protein called protamine to insulin slowed the absorption of the hormone, extending its effectiveness. This led to the creation and eventual commercialisation of Neutral Protamine Hagedorn (NPH) insulin. Bearing Hagedorn's name, it was the world's first long-acting insulin, which allowed patients to take fewer injections.
But Novo didn't like being outdone one bit. Novo chemist Knud Hallas-Møller spearheaded work on a new insulin formulation that didn't require any additives to prolong its effect. His efforts yielded the Lente (Latin for slow) series of insulins, which Novo would eventually commercialize in the 1950s. It provided sustained insulin action through a crystallized zinc formula, and just like Nordisk's NPH variant, it became widely adopted. Competition was driving innovation, and diabetics all over the world were reaping the rewards.
Novo continued to branch out, and after the aforementioned trip across the Atlantic to get some much-needed insight into penicillin production, it perfected its own method. By 1947, it had become one of the first companies to commercially produce a stable form of the drug and was looking to diversify even further. It would eventually go on to produce a wide array of antibiotics and biochemical products in the years to come. Nordisk, on the other hand, was laser-focused on improving insulin and treating diabetes, but would eventually join its twin company in expanding into other pharmaceutical areas.
By the 1950s, Novo and Nordisk were both well-established, substantial enterprises. In 1951, the Pedersen brothers made the decision to place their ownership shares into the newly created Novo Foundation. The brothers were nearing retirement, and to protect Novo's mission and independence after they were gone, they went down the same route that Nordisk had done during its founding. These two foundations would eventually merge along with the companies.
Scientifically, the decades following the Second World War saw both Novo and Nordisk expand beyond insulin and into new biotechnologies. In the late 1950s, both companies made continual improvements in insulin purity and delivery.
Novo introduced a new, purer version called monocomponent insulin. To make a long story short (and to spare you from half a page of medical terminology), it meant that insulin could be injected without the side effects that earlier preparations sometimes caused. Needless to say, a massive quality of life improvement for patients.
Both companies were also working furiously to find better ways to improve everything surrounding their medications. Some of these scientific breakthroughs were commercialized, while others laid much of the groundwork for future progress. All in all, Novo and Nordisk were trying to find the best possible way to treat diabetes, while also trying to outdo each other.
By now, Novo was extremely skilled in fermentation, given their work with penicillin, and leveraged this into other products. Nordisk was not far behind, and in the 1960s, both companies developed methods to produce various pharmaceuticals via microbial fermentation rather than relying on animal organs. Novo also continued down the beaten track of producing industrial enzymes, and both companies developed steroid hormones. The twin companies were no longer just insulin producers but were steadily becoming more and more diversified pharmaceutical companies.
Physically, the companies were growing as well. Novo had purchased a large tract of land in the Copenhagen suburb Bagsværd, and over the coming years built a campus of laboratories, offices, and production facilities. Nordisk was based in Gentofte, another suburb 15 minutes away by car. By the 1970s, little Denmark had two nearly identical companies that were competing against each other, and were leading the insulin push/innovation globally.
Get curated quality company deep dives every other week.
As the 70s made way for the 80s, diabetes treatment was on the cusp of a major breakthrough. The days of a diagnosis equalling a death sentence were long gone, but staying true to their ethos of driving scientific progress forward, both Novo and Nordisk continued to research. In the early 80s, they were chasing what at the time was the next step for diabetes treatment: human insulin.
We're once again going to simplify, since all of the medical terminology is something that we, for one, don't understand, and secondly, because you didn't come here to read us paraphrasing academic papers on amino acids. Novo and Nordisk were pursuing different paths to create insulin that was identical to what our bodies naturally produce. In 1982, Novo launched the world's first semisynthetic human insulin. Its researchers had devised a way to chemically convert the insulin from pigs into the exact human form. It made it easier for the body to absorb the insulin, cutting down on immune reactions and improving its action.
But Novo wanted to take it all a step further. Over in the U.S., other companies had begun producing human insulin through genetic engineering using bacteria. Novo poured money into the technology, and by 1987, it succeeded in making recombinant human insulin using yeast cells that had been genetically modified.
So what was the big deal, given that human insulin had already been produced? It meant that instead of using animal pancreases to produce insulin, it could now be manufactured in virtually unlimited quantities. Nordisk was also working on biosynthetic insulin and introduced its own version around the same time. By the late 1980s, “human insulin” had largely replaced animal-sourced insulin in much of the world.
Insulin remained the bread and butter for both companies throughout this period, but the late 1970s and 1980s saw further expansion. Nordisk had become one of the global leaders in treatments for hemophilia and was working on a new therapy for patients who had developed resistance to conventional treatments. Novo was also working on hemophilia treatments, and together with the Swedish researcher Dr. Ulla Hedner, it would introduce NovoSeven in 1996. The medication would go on to become the gold standard to control bleeding for certain patients who had previously been unreceptive to treatment.
Novo had a fantastic 1980s, not just in breakthroughs in insulin, but also in improving patients' lives. You've more than likely seen a friend or a family member use an insulin pen to quickly distribute a dose of insulin after a meal by injecting it. These are called pen injectors, and while the name might be somewhat unimaginative, it completely transformed how patients receive insulin.
Before these pen injectors, most people with diabetes took their insulin via bottles and syringes. While this might work well enough when you're at home, it was cumbersome to carry around and could easily draw more than a few looks when doing it at a restaurant or in the break room at work. In 1985, Novo introduced the NovoPen, the first insulin pen device. It was sleek, easy to use, and given its (as the name suggests) pen-like size, it was easy to carry around. It came pre-loaded with insulin cartridges, making injection easy, inconspicuous, and quick.

While not as life-changing as the first discovery of insulin back in the 1920s, it was a major, major quality of life upgrade and showcased yet again that Novo (and Nordisk, who quickly developed their own pen) didn't just care about making insulin. Its mission was to make living with diabetes as easy as it could.
By the end of the 1980s, Novo and Nordisk together had built a broad portfolio: insulin, oral antidiabetic agents, growth hormone, contraceptives, enzymes, antibiotics, advanced research programs in bleeding disorders, and more. Each was a sizable company by Danish standards, yet on the global stage, they were still relatively small players, often competing with much larger multinational pharmaceutical firms. This fact, along with ever-increasing R&D bills given the nature of modern biotech research, gradually pushed the two rivals toward an inevitable conclusion: they could achieve more together than apart.
Copenhagen suburbia had until now been big enough for the two of them, but as we reach the end of the 1980s, the arguments for keeping the companies separate were getting weaker by the day. They were located almost comically close to each other, chasing the exact same markets, and were recruiting from the same pool of Danish scientists. They had duplicated efforts in insulin research (which, surprise, surprise, isn't cheap), and as the cost of development soared, combining forces became increasingly logical.
When researching Novo Nordisk and looking at it with modern eyes, the fact that the two companies had remained separate for so long almost borders on self-sabotage. But we, nor you as a reader, sat in those boardrooms in the mid-1980s when informal talks around the subject were being held, without yielding anything. We haven't spent our career working for a company in a relatively small city in a small country with such a clear competitor, and where the rivalry has become so ingrained in the walls.
For both sides, it was simply unthinkable to suddenly wake up one morning and start working in a lab together with those you've been saying snide remarks about for your entire working life. There were deep cultural differences that stretched back to the 1920s, and personal feuds that were simply too large to overcome. The companies had spent their entire lives locked in a struggle against each other, competing for talent, patients, and markets. Novo and Nordisk were different, their separate workforces and leaders didn't particularly like each other, and that was just the way it was.
This fierce rivalry had however served them and patients around the world well. The two companies were constantly trying to push innovation forward and beat their neighbor, but as the 1980s were drawing to a close, it was becoming apparent that there was only one way to go into the future: together.
A new generation of leadership and a clear-eyed look at global competition helped overcome the barriers that had previously seemed impassable. A combined company could gain both scale and efficiency, and give it the chance to grow into one of the top players in pharmaceuticals globally, whereas separately, they would more than likely remain medium-sized niche companies. The arguments surrounding greater scientific, commercial, and financial strength, better global competitiveness, and a larger pool of resources for research eventually won out.
In January 1989, the boards of the Novo Foundation and the Nordisk Insulin Foundation (which held controlling stakes in the respective companies) issued a joint press release. They declared their intention to merge into a single Novo Nordisk Foundation, paving the way for a full corporate merger. The statement was met with shock, both in the organizations and in Denmark at large.
A historic era of rivalry was at an end, and the merger instantly created the world's largest insulin producer that could now leverage Novo's strong marketing and manufacturing with Nordisk's best-in-class research.
But a merger of this scale is not something that you complete in the course of a two-week agile sprint. Integrating the two workforces, moving everyone over to Bagsværd at Novo's campus, completing paperwork, and a million other things had to be done. But once the company found its stride, something that can only be described as extraordinary growth commenced.
As Novo Nordisk entered the 1990s as a unified company, it embarked on a period of vigorous global expansion and product innovation. One immediate priority was to strengthen its presence in the crucial U.S. market. It already controlled around 75% of the European market, but was looking to increase its presence across the Atlantic. It set up a subsidiary to take control of American sales and expanded its manufacturing facilities. Emerging markets in Asia and South America followed, with China being identified as a future core market
Product-wise, Novo Nordisk continued to innovate. It introduced pre-filled disposable insulin syringes, updated the NovoPen, launched an antidepressant, new hemophilia treatments, diabetes pills, and much more. All of this was done while the necessary investment required to maintain a technological edge was being made. By the turn of the millennium, Novo Nordisk's product range in diabetes spanned traditional human insulins, newer insulin analogs, oral antidiabetics, and delivery devices.
In 2000, Novo Nordisk made the decision to spin off its entire enzymes division into a separate company. For decades, Novo had run pharmaceuticals and industrial enzymes under one roof, but leadership decided that each would thrive better as independent, focused companies. This, combined with a number of other spin-offs in the 90s and early 00s, was part of a clear strategy: Novo Nordisk was to focus on its core strengths and become the global leader in diabetes care and biopharmaceuticals.
Under the leadership of President and CEO Lars Rebien Sørensen, who took the helm in 2000, and led by chief scientist Lotte Bjerre Knudsen (more on her in a second), the company doubled down on its mission to conquer diabetes and related chronic diseases. One of the most significant scientific endeavors of this era was Novo Nordisk's work on a new class of medications called GLP-1 analogs.
GLP-1 (glucagon-like peptide-1) is a hormone that humans naturally have and is responsible for natural insulin secretion. Researchers had hypothesized that harnessing GLP-1 could lead to effective treatments for type 2 diabetes, while offering benefits like weight loss and lower hypoglycemia risks as well.
As you may already be aware, that hypothesis proved to be correct.
The efforts were led by Lotte Bjerre Knudsen, and without her scientific efforts, we wouldn't be writing about Ozempic and Wegovy. Given the impact these two medications have had on both Novo Nordisk and millions of people around the world, we're going to have to forego our previous policy of avoiding explanations littered with medical terminology. But don't worry, the story of how GLP-1 was made into a viable drug is so interesting it's almost worthy of its own article.
Discovered in the 1980s, GLP-1 is a 30-amino-acid incretin hormone that stimulates insulin secretion and helps regulate blood sugar. Early studies showed that infusing the natural GLP-1 peptide in people with type 2 diabetes could normalize blood glucose levels. Now this sounds absolutely fantastic at surface level, and even the writer of this article can see that this could probably be helpful in treating diabetes.
Shockingly enough, the trained experts with decades of scientific experience at Novo Nordisk thought the same. But there's a catch: GLP-1 has an extremely short half-life. Just minutes after it's been administered intravenously, the effects have worn off. It's quickly broken up by an enzyme called DPP-4 and then flushed out by the kidneys. In other words, GLP-1 therapy was tantalizing, but someone needed to figure out how one could extend the hormone's lifespan in the body long enough for it to be a viable drug.
That someone would turn out to be a team at Novo Nordisk, led by Knudsen. She was a young researcher who interned in the department working on industrial enzymes, before transitioning to the diabetes research group. Early on, Knudsen and colleagues faced repeated setbacks trying to wrestle this fickle molecule into a usable drug.
By the late 1990s, Novo Nordisk management was close to pulling the plug on the GLP-1 project after years of frustration, more than likely large amounts of profanities in Danish, and inconclusive results. As Knudsen later recalled, she returned from maternity leave to find most of her team gone, and was bluntly told by a new R&D chief that the project had one last chance.
Faced with the do-or-die mandate, Knudsen homed in on a strategy that would come to define GLP-1 therapeutics: prolong the peptide's life by binding it to a carrier molecule. At the time, other approaches were also being explored by various teams – for example, the first GLP-1 mimetic drug to reach market was exenatide, approved in 2005, which cleverly used a DPP-4-resistant peptide from Gila monster venom. But Knudsen's focus was on modifying human GLP-1 itself to make it last longer in circulation.
There were three different avenues she and her team considered:
Protect the hormone: shield it from DPP-4 and clearance mechanisms (for instance, by binding it to a larger molecule).
Remove what destroys it: eliminate or evade the enzymes (like DPP-4) and processes that break it down.
Make the molecule more stable intrinsically: alter GLP-1's structure so it resists enzymatic cutting and clearance.
It was ultimately a combination of the first and third approaches that did the trick. Drawing inspiration from the body's own albumin, an abundant blood protein with a naturally long half-life, her team hypothesized that attaching a fatty acid chain to the GLP-1 molecule could hitch it to albumin and effectively “hide” it from DPP-4. Albumin is produced in large quantities and circulates for weeks, ferrying fatty acids and other molecules through the blood. By reversibly binding a therapeutic peptide to albumin, one could dramatically extend GLP-1's presence in the bloodstream. In 1998, Novo researchers published the first attempt. While a step forward, it was unstable and not suitable as a drug.
By the early 2000s, after exhaustive experimentation, Knudsen and colleagues achieved a breakthrough. They engineered a modified GLP-1 analog that would become known as liraglutide. After being selected as the lead candidate around 2003, liraglutide advanced through preclinical testing and into clinical trials.
By 2010, liraglutide (under the brand name Victoza) was approved for type 2 diabetes, becoming the first long-acting GLP-1 analog in the world. and Lotte Bjerre Knudsen and her team had managed to do what many thought impossible. We're going to return to Knudsen and the research behind the next step in GLP-1 treatments: Ozempic and Wegovy.
Given the way that Ozempic and Wegovy have impacted Novo Nordisk (and its stock price), and that we've just introduced their predecessor, we're about to enter into the modern era of the company. But during the aforementioned CEO Sørensen's tenure, the core focus on insulin remained the same as it had always been.
The company's share of the global insulin market continued to grow, especially in emerging economies where Novo Nordisk continued to expand. During this period, Novo Nordisk was the largest insulin maker globally, supplying nearly half of the world's insulin by volume. A single production site, the company's sprawling plant in Kalundborg (originally opened in 1969), was by itself turning out roughly 50% of the world's insulin supply by 2000.
Sørensen's tenure was also marked by a long series of initiatives surrounding global health. In 2002, Novo Nordisk's shareholders approved an extraordinary initiative: taking a portion of the company's profits to establish the World Diabetes Foundation (WDF). It was set up as an independent nonprofit (Novo Nordisk does have representation on its board), with the mission to improve diabetes care in poor countries. In 2005, it created the World Haemophilia Foundation, with the same mission.
By the time Sørensen stepped down in late 2016 (after 34 years at the company and 16 as CEO), Novo Nordisk had more than quadrupled its revenues since the turn of the century and firmly established itself as a global powerhouse in diabetes care and biologic drugs.
In 2017, Lars Fruergaard Jørgensen became Novo Nordisk's new chief executive, only the fourth person to hold the role as CEO since the merger in 1989. He took the reins just as Novo Nordisk was expanding beyond diabetes into a closely related and rapidly growing field: obesity treatment. The groundwork for this pivot had been laid by Victoza (liraglutide), which, in addition to treating diabetes, showed weight-loss effects. Novo Nordisk developed a higher-dose version of liraglutide specifically for obesity, branded Saxenda, which gained approval in 2014.
But an even bigger leap came from the company's next GLP-1 drug: semaglutide.
Semaglutide was the work of Knudsen and her team. Liraglutide was administered daily, but the researchers at Novo Nordisk were looking to find a way to administer GLP-1 on a weekly basis. Semaglutide was the answer. Building directly on the liraglutide design, the team modified the molecule to extend its half-life further while maintaining potent GLP-1 receptor activity.
Semaglutide entered clinical trials and quickly proved its worth, and by 2017, it was approved as Ozempic for type 2 diabetes. Perhaps most dramatic was semaglutide's effect on body weight. In trials for obesity, weekly semaglutide led to unprecedented results: In one direct comparison of their effects on appetite, liraglutide was shown to cut food intake by about 15%, whereas semaglutide reduced it by up to 35%.
Novo Nordisk wasted no time testing semaglutide specifically for obesity, and in June 2021, the high-dose injectable semaglutide was approved for chronic weight management under the name Wegovy. Its launch marked Novo Nordisk's full entry into the obesity pharmacotherapy market – a market that soon exploded in size as these new GLP-1-based medications showed unprecedented efficacy (15% or more weight loss in many patients).
The market response to the introduction of Ozempic and Wegovy was immediate: Ozempic quickly became one of the best-selling diabetes drugs in the world. By 2024, Ozempic sales were over $18 billion annually and still growing. Demand was so high that periodic supply shortages occurred globally.
The twin successes of Ozempic and Wegovy sent Novo Nordisk's revenues and stock price soaring. Novo's public image also shifted: no longer was it seen merely as an insulin company or even just a diabetes company; it was now the global leader in tackling obesity, a condition affecting over 650 million people worldwide. Internally, the company reframed its purpose as going “beyond diabetes” to solve broader chronic health challenges.
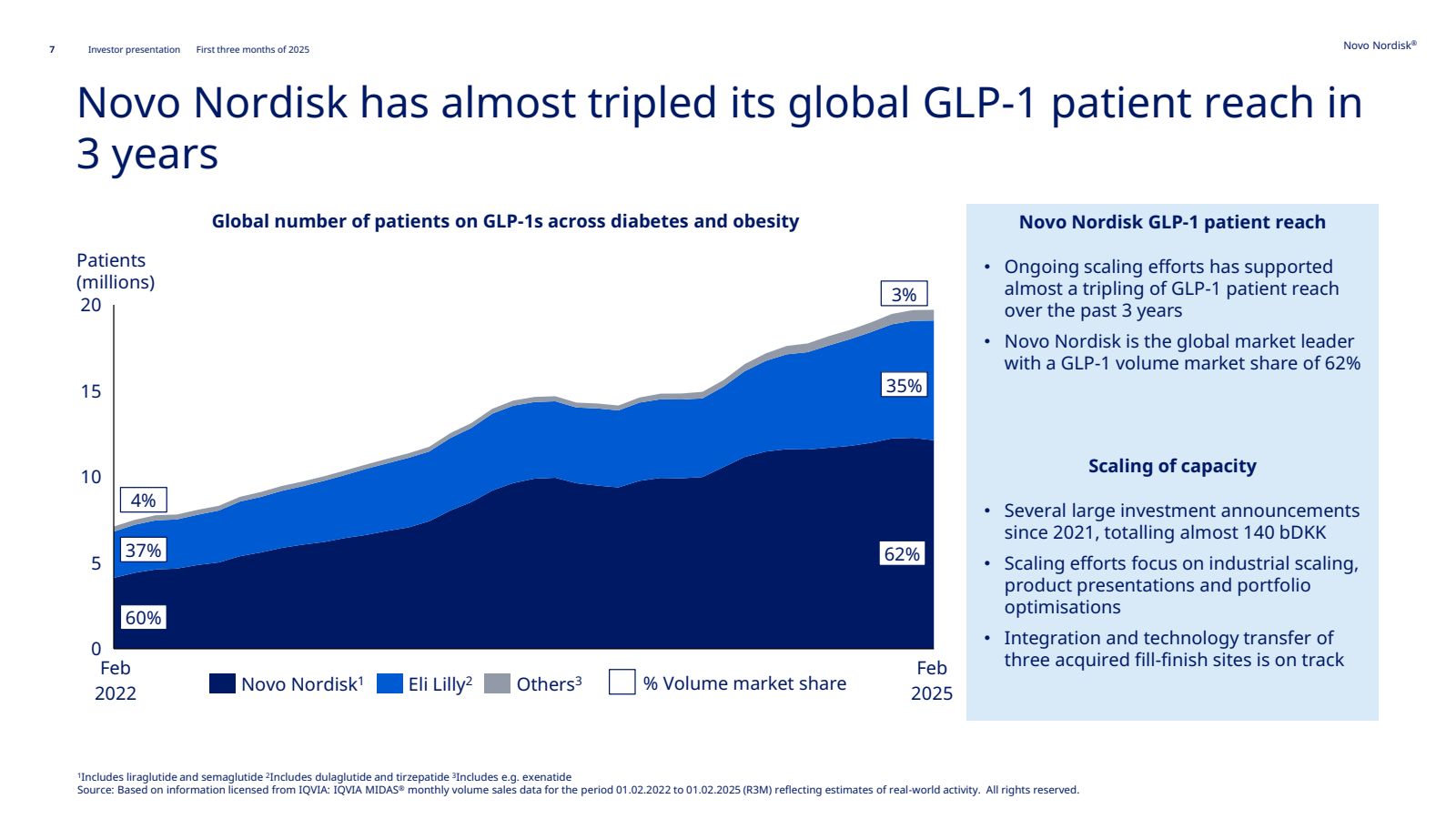
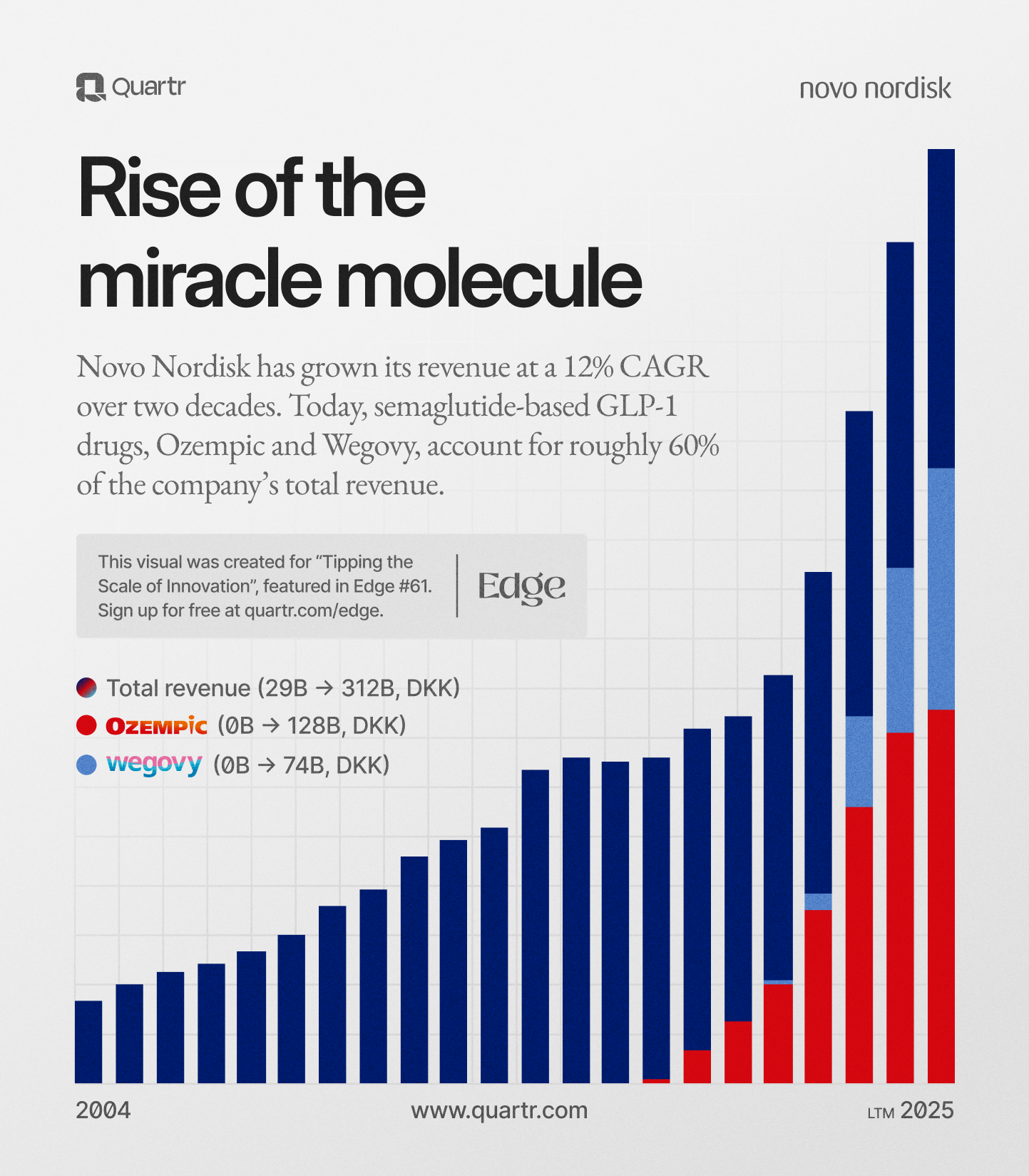
Weight-loss drugs became the majority of Novo's growth: in the first half of 2023, Novo's profits jumped 45% year-on-year, and most of that growth came from Ozempic and Wegovy, which together made up 55% of all of Novo Nordisk's revenue in 2023. By the first nine months of 2024, Wegovy sales were up 42% and Ozempic 54% year-on-year, and Novo reported holding a stunning 74% share of the entire global market for anti-obesity medications. In just a few years, Novo Nordisk had come to define the entire market.
The stock price followed.
But as you may be aware, Novo Nordisk and its stock have fallen from the heights it was at just a couple of years ago. To understand why, we're going to take a look at the modern business, and why the growth initially offered by Ozempic and Wegovy hasn't proven sustainable.
We're about to get into the nitty-gritty of how the company works, and in order to understand that, we need to take a closer look at the foundation. Both the founders of Nordisk and Novo established their companies under the ownership of a foundation, which like previously mentioned, merged when the companies did. Both the Novo and Nordisk foundations were set up to ensure stable, long-term ownership of the insulin enterprise and to channel some profits into scientific and humanitarian causes.
Today, the Novo Nordisk Foundation is integral to how the company operates and plans its future. The Foundation (via its holding company Novo Holdings A/S) owns all of Novo Nordisk's unlisted Class A shares, which carry supervoting rights. Although the Foundation's equity stake in Novo Nordisk is roughly 28%, it controls about 75-77% of total voting rights in the company.
In practical terms, this makes Novo Nordisk a controlled company, with the Foundation holding veto power over major decisions and takeovers. The Class A shares are not publicly traded (to prevent outside takeovers), whereas Class B shares are traded on the Copenhagen Stock Exchange. Its place in the Copenhagen Index (and role in the Danish economy), is something we'll discuss further in just a moment.
The benefits of this model have been significant for Novo Nordisk's business: it shields the company from short-term market pressures and hostile takeovers, allowing management to focus on long-term strategy. It also provides a financial safety net that Novo Nordisk can lean on during downturns or when funding expensive research. The foundation's presence has reinforced a culture of “innovation first” rather than a “quarterly earnings above all” mindset.
Novo Nordisk is, at its core, a pharmaceutical manufacturer that makes money by developing, producing, and selling medications. The bulk of its revenue comes from a relatively small number of blockbuster products in the diabetes and obesity space, with additional contributions from treatments for rare disorders.
Let's break down the main components of Novo's business model and see where the company generates revenue:
This includes insulins and GLP-1-based drugs for diabetes. In 2024, diabetes care brought in about $30 billion, roughly 71% of Novo's sales. Insulin products still contribute a significant portion of this, with a broad portfolio ranging from older human insulins to modern analogs.
However, the growth in diabetes care is almost entirely due to the GLP-1 drugs. Sales of GLP-1 medicines for Type 2 diabetes grew 22% in 2024 to $24 billion, making them the largest category within Novo. By contrast, insulin sales are growing slowly or even stagnating in some markets due to competition and pricing reforms. Novo's strategy has been to offset insulin price pressure with volume (targeting more patients in emerging markets) and by shifting customers to products like ultra-long-acting insulins that still hold patent protection.
This is essentially the products Wegovy and Saxenda, and Obesity care has become the fastest-growing segment for Novo Nordisk. In 2024, obesity product sales reached roughly $10 billion, up 56% from the prior year.
Novo has a smaller segment catering to rare chronic conditions, notably hemophilia and other bleeding disorders, and growth hormone deficiency. Key products include NovoSeven (for hemophilia with inhibitors), NovoEight/NovoThirteen (hemophilia factors), and Norditropin (human growth hormone). In 2024, rare disease products represented 6.4% of total sales.
Novo Nordisk's most important markets are geographically diverse, but one towers above all: the United States. The U.S. is the world's largest pharmaceutical market and has been incredibly lucrative for Novo Nordisk. In recent years, North America (mostly the U.S.) comprised roughly 60% of Novo Nordisk's sales. Specifically, in 2024, North America sales grew 30% to around $27 billion, while International sales grew 17% to $18.5 billion.
The U.S. alone contributed more than all other countries combined. This imbalance reflects not just higher demand but also higher pricing in the U.S., where drug prices are market-driven and can often be 2-3x what they might be in Europe for the same drug.
For Denmark, Novo Nordisk's journey from a small insulin lab to a global biotech leader has been a source of pride and a source of prosperity. Denmark has roughly 6 million inhabitants, and at its peak in 2024, Novo Nordisk's market cap was larger than the country's entire GDP. It paid $3.8 billion in taxes last year, its ecosystem now accounts for roughly 10% of Denmark's GDP when indirect effects are included, and around 40% of the country's exports.
Novo Nordisk's heft is just as evident on the Copenhagen stock exchange as it is in economic data. The company is a cornerstone of the OMX Copenhagen 25 index (at the time of writing it makes up roughly 10%. In 2024, it was around 16%), and its stock movements set the tone for the entire Danish market. Its inclusion in the broader index also means that millions and millions of Danes are exposed to the stock indirectly through pension funds, index funds, and similar investment vehicles, regardless of whether or not they directly own any stock.
While saying that Novo Nordisk is in serious trouble might be somewhat exaggerated, the current situation is vastly different from the highs of last year. With the stock taking a tumble after adjusting guidance (we're talking about this in-depth in just a moment), the forecast for the Danish economy this year has had to be adjusted. Nykredit, one of Denmark's largest banks and financial services companies, projects that the GDP will grow by 0,9% in 2025, down from the previous projection of 3,5 %. Exports are projected to decrease by 1,9% instead of increasing by 3,9% as previously forecasted.
Denmark's fortunes are, for better or worse, extremely tied to how well Novo Nordisk performs. This is, needless to say, great when the stock is rallying, but it also carries risk. It's hard to overstate the impact that Ozempic and Wegovy have had on the Danish economy, and while officials and politicians in parliament claim that there is no overreliance on Novo Nordisk, the numbers speak for themselves. We'll leave the question of whether or not Denmark is over-exposed, but a large portion of its fortunes are tied to a single pharmaceutical firm.
One of the most characteristic traits of Novo Nordisk's business is its unwavering focus on research and development (R&D). In practice, Novo Nordisk typically reinvests about 13–15% of its annual revenue into R&D programs. In 2024, for instance, it spent around $3.5B on R&D. These funds fuel a broad pipeline of projects, not only in the company's core areas of diabetes and obesity, but also in adjacent fields like cardiovascular disease, kidney disease, and rare disorders.
Novo's R&D ethos is deeply patient-centric as the company strives to create treatments that improve patients' lives in meaningful ways, while also researching incremental improvements. In doing this, it strikes a balance between making existing treatments better, safer, more convenient, and disruptive innovation.
A good example of incremental improvement is the continuous fine-tuning of insulin analogues, with a disruptive example being semaglutide. The incremental keeps its current products at the top of their game, and the disruptive ensures its future beyond current patents. The company needs both kinds.
It's also worth noting that Novo's R&D spending, while large in absolute terms, is very focused. Unlike pharma conglomerates that research everything from oncology to immunology, Novo Nordisk concentrates on what it knows best. This focus means their scientists develop deep expertise and can often be first to market. It also means R&D dollars aren't wasted in areas where Novo doesn't have a competitive edge. While many research projects fail, others end up creating a whole new market for the company to dominate. It was the case with GLP-1, and who knows? Researchers are sitting in a lab at Novo Nordisk's campus right now working on what might just be the next blockbuster.
In the pharmaceutical world, a drug patent is like a 20-year monopoly on an invention, when a company exclusively sells its drug and recoups hefty R&D. A “patent cliff” refers to the drop that occurs when this exclusivity ends and generic competitors rush in. It's not uncommon for a blockbuster drug's sales to plummet by 80–90% within the first year or so after a patent expires.
As patents inch toward expiry, companies ramp up R&D efforts, often tweaking existing drugs or formulating new ones to extend their market lead
Yet, innovation on demand is no simple feat. Drug development is lengthy, expensive, and fraught with failure. The impending loss of a cash-cow drug adds pressure to the process. Companies might also look outward: licensing promising compounds from smaller biotech firms or acquiring competitors to fill gaps in their pipeline. A well-timed breakthrough can mean a seamless transition to a new revenue stream, while a miss can mean a painful drop at the cliff's edge.
Why do these patent timelines matter so much for Novo Nordisk? The answer lies in how critical Ozempic and Wegovy have become to the company's fortunes. The heritage and base might be insulin, but GLP-1 is the growth driver. But at the same time, the patent cliff is at this point the least of Novo Nordisk's worries, given what the competition looks like.
In November 2023, U.S. regulators approved Eli Lilly's tirzepatide (branded Zepbound for obesity), giving Lilly a direct rival to Wegovy. Head-to-head trials showed patients lost more weight on tirzepatide than on semaglutide and by early 2025, prescription trends confirmed Novo was losing ground.
Meanwhile, new competitive threats continued to surface: in 2025, Lilly unveiled impressive results for an oral GLP-1 pill (orforglipron) that in trials matched injectable Ozempic's efficacy, news that instantly added ~$100 billion to Lilly's market cap. Lilly is also advancing retatrutide, a next-generation “triple agonist” injection that showed a striking 24% average weight loss in early trials.
Beyond Lilly, virtually every major pharmaceutical player is now chasing the obesity market. Over 120 drugs are in development for obesity across the industry, including candidates from Pfizer, Amgen, AstraZeneca, Roche, and others. This wave of R&D means Novo will face a crowded field in the coming years.
A very pragmatic challenge has also been simply making enough products. The demand for Ozempic and Wegovy has been so high that Novo Nordisk's production capacity became a limiting factor. The company had to prioritize certain markets and delay some launches because it couldn't supply everyone immediately. These shortages had two important side effects: revenue was left on the table as Novo simply couldn't fill all the prescriptions being written, and a gray-market solution emerged in the form of compounding pharmacies.
In the U.S., specialty compounding pharmacies began offering “cheaper replica” versions of semaglutide injections, using the same active ingredient as Wegovy/Ozempic. Under U.S. law, pharmacies are generally barred from copying approved drugs, but an exception exists when the brand-name product is in short supply. Taking advantage of Wegovy's shortage listing, compounders stepped in to sell semaglutide formulations at lower prices, often via telehealth and wellness clinics, with Hims & Hers being one of the more prominent providers.
By early 2025, Novo estimated roughly 30% of all semaglutide volume in the U.S. was being provided by these unofficial channels. We're going to talk more about the stock in a second, but here's what Novo Nordisk had to say on the matter:
"The change in sales outlook for 2025 is driven by lower growth expectations for the second half of 2025. This is related to lower growth expectations for Wegovy in the U.S. obesity market lower growth expectation for Ozempic in the U.S. GLP-1 market as well as lower-than-expected penetration for Wegovy in select IO markets. The lower growth expectation for Wegovy in the U.S. obesity market reflects the persistent use of compounded GLP-1."
– CFO Karsten Knudsen, Guidance update, July 29th, 2025 (sourced with Quartr Pro).
To understand why the stock has gone down over 60% from its highs, we must first understand why the stock went up. And while it, at a surface level, can be boiled down to “new drug is popular and is selling a lot”, it is a little more nuanced than that.
First, Novo's financial performance consistently beat expectations, leading management to raise guidance repeatedly. Since Wegovy's 2021 launch, Novo has habitually upgraded its annual sales forecasts multiple times per year as demand outstripped supply, feeding investor optimism. Second, the market envisioned a vast new revenue stream in global obesity treatment. Analysts projected the obesity drug market could exceed $100–150 billion annually within a decade, and as the first mover, Novo was expected to capture a dominant share.
But cracks began to appear in the narrative that Novo Nordisk was unstoppable, and that its first-mover advantage was so large it would take years and years for the competition to catch up. As we've just been over, a few years after Wegovy hit the market, competition was already incredibly fierce. To add to this, Novo Nordisk's pipeline wasn't the home run many had counted on it being.
The most notable disappointment was CagriSema, an experimental obesity drug. Novo had billed CagriSema as a successor to Wegovy with even greater efficacy, setting bold expectations (a 25% weight loss goal). Unfortunately, when late-stage trial results were revealed in December 2024, CagriSema fell short of the hype – patients lost 22.7% of their weight on average, a strong result but below Novo's target, and the combo caused slightly more nausea than Wegovy. Investors, who had “baked in” CagriSema as a major growth driver, reacted sharply as Novo's shares plunged. Compounding the issue is the fact that, if approved, CagriSema won't reach the market until 2027.
Underpinning all the above factors is a clear shift in investor sentiment. Novo Nordisk's financial results, while still strong in absolute terms, have begun to underperform the market's prior lofty expectations. The company's own forecasts tell the story. After two years of 30%+ revenue growth, Novo in early 2025 guided for a much lower 16–24% sales growth in 2025. By mid-2025, even that proved optimistic and on May 7, 2025, Novo cut its 2025 outlook and announced it expected only 8–14% sales growth and similarly reduced profit growth.
The immediate trigger for the cut was softer U.S. GLP-1 sales, due in part to the aforementioned compounding issue and a plateau in Wegovy prescriptions by early 2025. But more broadly it reflected that growth was slowing from “breakneck” to merely “strong” – a natural progression as the base of revenue gets larger and competition intensifies.
The stock reacted brutally to the guidance cut. In July 2025, when Novo formally reported the lower outlook, the stock tumbled 20% and over $57 billion was wiped off its market cap.
Investors are also looking more critically at Novo's concentration of revenue. Over 90% of Novo Nordisk's sales now come from its diabetes and obesity care segments. This heavy reliance on GLP-1-related products is a double-edged sword – fantastic when those products are growing, but a vulnerability if growth stalls. At 14x its trailing twelve-month earnings, Novo is now valued similarly to an “ordinary” large pharmaceutical company like AstraZeneca, rather than a hyper-growth outlier.
To sum it all up into one sentence: Novo lacks a near-term follow-up to Wegovy at a time when competitors are charging ahead with new products. The company now finds itself having to play catch-up in innovation, where before it set the pace. But despite the stock's collapse, Novo's current business remains robust. The company is still growing double-digits and generating billions in profit, and Wegovy and Ozempic continue to see strong demand.
Novo Nordisk is also bringing in a new CEO. Jørgensen, who had overseen the explosive growth of GLP-1, announced that he and the board had agreed he would step down in May of 2025. He stepped down following internal and external concerns that Novo Nordisk was (rightly so) losing its first-mover advantage. Effective as of August 7th, 2025 (the day before the publication of this article), the company will be led by Maziar Mike Doustdar.
Doustdar has served as executive vice president and head of international operations since 2015, and here's what he had to say when introducing himself in late July:
"We need to increase the sense of urgency and execute differently. But we'll do that by building on the core strength that makes this company so unique. I take this job very seriously. You can expect me to be a CEO that combines strategic clarity with operational urgency. Soon I'll be working closely with my management team, the Board and the entire organization to move forward. We will sharpen our focus and move faster. We will operate more efficiently. We will advance our pipeline and keep pushing the boundaries of innovation and we will invest to accelerate growth and deliver shareholder value. That is my promise to you."
– Novo Nordisk CEO Maziar Mike Doustdar, Guidance call, July 29th, 2025 (sourced with Quartr Pro)
Will Doustdar be able to revive Novo Nordisk's presence in the U.S.? Will the company be able to challenge Eli Lilly with new products? Will the stock bounce back to its highs? Time will tell.
Since that trip to Toronto, Novo Nordisk has been guided by one mission: improving the lives of patients. Human insulin, improved delivery devices, GLP-1, and everything have all been absolute gamechangers for people living with diabetes. And yes, more often than not, this has also been a very profitable thing to pursue.
Scientific research has always been the cornerstone of the entire business, and that’s not something that’s changing anytime soon. Will the researchers in Bagsværd come up with a new blockbuster soon? We don’t know, but one thing is certain: they’ve done it before.
Explore our platforms
Leading companies and financial institutions worldwide rely on Quartr to make better decisions faster.
Desktop
API
Mobile
)
)
)